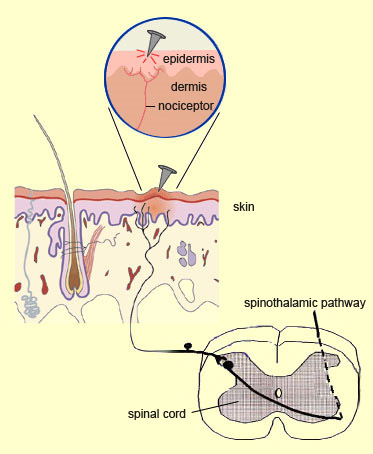
The surface of the body—the skin—contains
very large numbers of the free nerve endings known as nociceptors, which is why
it is so sensitive to pain. These nociceptors are located both in the epidermis
(the surface layer of the skin) and the dermis (the deep layer) and are concentrated
in the parts of the body that are the most exposed to injuries, such as the fingers
and toes. That is why it hurts more to get a piece of glass stuck in your finger
or toe than in, say, your chest or your shoulder.
The muscles,
protected by the skin, contain fewer nerve endings, and they are spaced more widely
and discontinuously. That is why muscle aches and pains are more diffuse and harder
to locate.
The walls of the blood vessels (arteries and
veins) are more richly innervated; the free nerve endings that are sensitive to
nociceptive stimuli are located in the inner layers of the blood-vessel walls.
In the bones, most of the free nerve endings are located
in the marrow and the periosteum, where they form a regular network. Anything
that damages the structural integrity of a bone, especially a serious injury such
as a fracture, will therefore cause pain.
In the joints,
pain receptors are located mainly in the capsule, the synovium, the ligaments,
and the tendons. These receptors can be activated either mechanically (tears,
strains, etc.) or biochemically (for example, in inflammatory processes such as
arthritis.
The internal organs, protected by the skin,
muscles, and bones, have even fewer nerve endings than the muscles. The free endings
in the internal organs are distributed loosely and very unevenly, which is why
pain in these organs is often vague and hard to locate, be it the simple discomfort
of indigestion or the violent pain of a kidney stone.
The internal organs
most highly innervated with nociceptors are mostly the ones that are hollow (such
as the intestines, bladder, and uterus). Because these organs are the internal
extension of the outside environment, they are more likely to come into contact
with potentially hazardous agents and therefore require proper monitoring. Conversely,
solid organs, such as the lungs, liver, and spleen, have fewer free endings and
are not highly sensitive to pain. Hence, they can deteriorate without the individual’s
becoming very aware of it.
MOLECULES THAT PRODUCE PAIN
The sense of touch originates
in specialized receptors located in the skin. These mechanoreceptors are
sensitive both to pressure and to light to moderate stretching. They send messages
through the neurons, and the central
nervous system interprets these messages as tactile sensations. But when the
mechanical pressures on a body tissue become so strong that they threaten its
integrity or actually damage it, then the pain receptors, also known as nociceptors,
take over.
The
nociceptors are free nerve endings: axon
tips that have no myelin
sheath. They are the highly ramified terminations of A
delta fibres and C fibres and are found not only in the skin, but also in
muscles, blood vessels, joint, bones, and internal organs (see sidebar)—in
short, practically everywhere in the body except
the brain itself! Thus, conceptually, a nociceptor refers more to a function
(that of feeling pain) than to a specialized kind of receptors (as is the case
with mechanoreceptors).
Nociceptors can be activated not only by
mechanical stimuli such as pinching, piercing, or biting, but by all kinds of
other stimuli that can potentially harm body tissues. Examples include extreme
temperatures (see sidebar), electrical shocks, hypoxic conditions (lack of oxygen),
or exposure to toxic substances . Some nociceptors are more sensitive to one kind
of stimulus rather than to others, but most nociceptors are polymodal, meaning
that they can respond to more than one kind of stimulus.
Regardless
of the kind of stimulus, it much reach a certain intensity before it can activate
the nociceptors (see sidebar), because their activation threshold is higher than
that of mechanoreceptors. Hence, by modulating their response according to the
intensity of the painful stimulus, nociceptors can encode this intensity. The
activation threshold of nociceptors in the skin represent the threshold at which
the individual can perceive the sensation of pain.
The
structures that let nociceptors sense such a wide range of painful stimuli consist
of various
types of ion channels located in their cell membranes. Some of these stimuli
are direct, such as strong mechanical pressures that deform the membranes and
trigger nerve impulses—for example, when you step on the point of a thumbtack,
but it does not pierce your skin.
But if you step on
a tack and it does pierce the skin, then the damaged cells locally release certain
chemicals that indirectly stimulate the nociceptors as well. Some of these
“algogenic” (pain-inducing) molecules released by the damaged or inflamed
tissue are enzymes such as bradykinin, while others are neurotransmitters
such as serotonin,
and others are hormones such as prostaglandin. Pain signals can also be generated
by an injury to a nerve fibre.
When subjected to strong
or repeated pain stimuli, nociceptors undergo sensitization
phenomena that lower their response threshold, increasing the number of nerve
impulses and the sensation of pain thus produced.
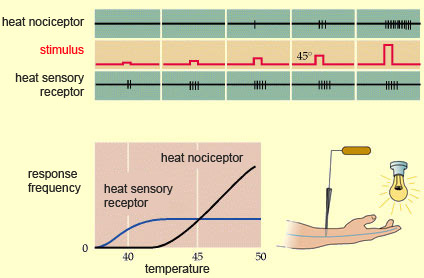
Painful sensations of heat are not produced by
excess activity of the same receptors that produce comfortable sensations of heat.
Instead, researchers have clearly shown, there are heat nociceptors that are separate
and distinct from ordinary heat sensory receptors. When the temperature of a heat
stimulus is increased gradually, the activity of the heat sensory receptors increases
proportionately up to a temperature of about 45°C, at which point this activity
levels off. In contrast, heat nociceptors don’t become active until the
temperature reaches 40°, but then their activity increases in proportion to
the heat, without reaching a plateau.
And
45°C is just about the temperature at which proteins in the body begin to
deteriorate, the body tissues begin to be damaged, and people begin to describe
a sensation of heat as painful. But of course, various
factors can shift the pain threshold by a few degrees.
The terms “opiates” and “opioids”
do not mean entirely the same thing.
Medications and other substances are
called opiates when they contain opium or any of its derivatives,
such as morphine or codeine. Opiate molecules are alkaloids, rather than peptides,
and come from a source outside the human body (poppy seeds or synthetic compounds).
The term opioids, on the other hand, refers to a group
of peptides that are endogenous to the body and that exert a physiological effect
similar to that of morphine. But, in a somewhat circular way, this expression
also tends to be used to refer to any substance—natural or synthetic, peptide
or not—that acts on what are referred to as the body’s opioid receptors.
Shortly after the discover of natural opioid
substances in the brain, people began to associate them with the phenomenon of
the “runner’s high”—the intense feeling of well-being
that many long-distance runners experience as they cross the finish line. But
this same euphoria can also be experienced by anyone who engages in moderately
strenuous physical activity for 20 or 30 minutes.
But scientists had remained
skeptical about the role of endogenous morphines in producing the runner’s
high, among other reasons because in experiments, administering opioid-receptor
blockers such as naloxone failed to prevent the subjects from experiencing this
sensation.
Some scientists even offered an alternative explanation: that
this mood change was actually attributable to another family of molecules, called
endocannabinoids, the body’s endogenous cannabis.
Like endorphins, endocannabinoids
produce their effects by binding to their own specific receptors in the brain—the
same ones as THC, the active ingredient in cannabis. Endocannabinoids help to
modulate pain. They also induce euphoria, and because their concentration in the
body was observed to increase after sustained exercise, researchers hypothesized
a connection between these substances and runner’s high.
However,
a study published by a group of German researchers in 2008 shifted the focus back
to endogenous opioid peptides as the source of runner’s high. First the
scientists used a psychological test to assess the mood of 10 human subjects,
all of them experienced runners. Then the researchers injected the subjects with
a radioactive substance that would reveal the presence of endorphins in their
brains in images produced by the brain-scanning method known as positron emission
tomography (PET scanning).
Next, the 10 subjects went out running for two
hours. When they got back, their mood was assessed once again, and the distribution
of radioactivity, and hence of endorphins, in their brains was determined by PET
scan. What the researchers found was that the more intense the subjects’
measured feeling of euphoria, the more endorphins were observed in a part of the
brain associated with the emotions: the limbic
system and the prefrontal
cortex.
This study has not identified
the precise
type of endorphin involved in runner’s high, and further research
should be done to make this distinction, because there are so many different types
of endorphins, and their effects vary. But an important connection does now seem
to have been established: the same substances that have the ability to reduce
our perception of intense pain also come into play to offset,
and even reverse, the discomfort caused by sustained physical effort.
MOLECULES THAT REDUCE PAIN
For many centuries,
people have been using opium, and various substances derived from it, such as
morphine, to relieve pain. The virtues of opium are praised in very early written
records, including the cuneiform writing of Sumeria and early Chinese ideograms.
But it was not until the 1970s that scientists learned that the human brain also
produces its own endogenous morphines. The story of the many discoveries that
led to this finding is fascinating in several respects.
First
of all, from a scientific standpoint, the researchers made some canny deductions
that enabled them to build evidence rapidly. Second, from a technical standpoint,
the researchers showed amazing ingenuity and determination, because they had to
isolate molecules that occur in very low concentrations in the brain. Lastly,
in terms of the sociology of the scientific community, this research effort was
remarkable, because it pitted various laboratories in a genuine race against one
another while at the same time requiring them to collaborate.
At
the start of this effort, scientists knew that opium and its derivatives —substances
derived from a plant—had a certain effect on the bodies of animals. In general,
for a molecule to affect a cell’s activity, that molecule must bind to receptors,
which are usually located in the cell’s membrane. And it is the binding
process that, like
a key opening a lock, opens the way to a cascade of biochemical phenomena
that have a physiological effect—in this case, an analgesic (pain-killing
one).
Thus, the first deduction that researchers made,
in the early 1970s, was that for these plant-derived opiates to act on animal
nerve cells, those cells must have receptors for opiates, just as they had been
shown to have for other
neurotransmitters. This deduction marked the start of the hunt for opiate
receptors, at a time when neurochemistry, the scientific discipline that now deals
with such matters, had scarcely begun to emerge.
Convinced that the highly specific effects
of morphine (contraction of the pupils,
depressed heart rate, reduced perception of pain, and so on) could be produced
only if the brain had specific receptors for it, U.S. scientist Solomon Snyder
began his research with the most direct approach: he placed radioactive morphine
in direct contact with neurons and then attempted to see whether any radioactive
molecules had become bound to them. If any had. this was a sign of the presence
of receptors on the neurons.
Unfortunately,
Snyder found no such molecules bound to the neurons, even when he repeated the
experiment with heroin
instead of morphine. While the rest of the scientific community was starting to
doubt whether opiate receptors even existed, he and his graduate student, Candace
Pert, tried their luck one last time, but with a substance called naloxone
that was known to block the effects of opiates.
And
this time, their luck changed: the radioactive naloxone did remain bound to the
neurons! This confirmed the earlier hypothesis that naloxone blocked the effects
of morphine by binding to receptors, and most likely to the receptors for morphine
itself. With this finding and some further investigation, the researchers realized
that in contrast to naloxone molecules, which block receptors by literally becoming
trapped in them, morphine and heroin molecules act by binding to receptors for
a very short time—too short a time to be detected.
Other researchers, such as Eric
Simon and Lars Terenius in 1973, also published similar observations
confirming the presence of opiate receptors in the central nervous system. These
findings generated a great deal of excitement in the field, because the presence
of opiate receptors almost automatically meant that the brain must naturally produce
some opiate-like substance to bind to them. In other words, it seemed extremely
unlikely that such specific locks would have evolved in the human brain without
the keys to open them also being present there (as opposed to keys that had evolved
by pure chance in the plant kingdom).
This
idea that morphine might simply be mimicking the effects of a substance already
present in the body had been in the back of the mind of several scientists who
who had worked on isolating the receptor. But it had been especially well defended
by the German-born biologist Hans Kosterlitz.
Kosterlitz,
working at the University of Aberdeen in Scotland, encouraged the assistant director
of his laboratory, John Hughes, to demonstrate the existence of this endogenous
morphine. Easy to say, but harder to do, with the tools available at the time.
Hughes therefore chose a kind of “morphine detector” that was available
to him: the vas deferens of the mouse, because it was already known that the contractions
of this tissue were inhibited by morphine binding to specific receptors. The idea
was to apply brain extracts to prepared samples of this tissue, and see whether
the contractions then ceased.
The problem was that some substances can act at
concentrations as low as the equivalent of 1 gram per 10 million litres of water.
The chances of success therefore seemed equally infinitesimal, and Hughes had
to prowl the slaughterhouses of Aberdeen to collect thousands of pig brains for
his laboratory. There he removed certain brain structures, ground them up, concentrated
them, and applied them to the mouse vasa deferentia.
In
1973, Hughes found some indications of the presence of an endogenous substance
capable of binding to opiate receptors, as did the the laboratory of Lars Terenius
in Sweden. These preliminary results were communicated in May 1974. Then, in December
1975, Hughes and Kosterlitz published the structure of two substances that they
named enkephalins,
from the Greek for “in the head”. Both of these substances were peptides:
small proteins
formed from just a few amino acids.
Specifically, each of these two enkephalins comprised a sequence of five amino
acids, and only the last amino acid in the two sequences was different: methionine
in the case of met-enkephalin, and leucine in the case of leu-enkephalin.
In
1976, the teams of Choh Hao Li and Roger Guillemin isolated some
longer peptides, endorphins,
that also were capable of binding to opiate receptors. Subsequently, many more
endogenous opioid peptides, such as the dynorphins,
were isolated, so that by 1992, some 20 such substances had been identified.
In 1971, John C. Liebeskind and his colleagues
published an article containing some strange observations: stimulating a midbrain
region called the periaqueductal
grey matter produced pain in laboratory animals,
but ceasing the stimulus or reducing its intensity had an analgesic (pain-relieving)
effect. This article also suggested that this latter effect was analogous to that
of opiate medications. They confirmed their intuition the following year, when
they showed that this analgesic effect produced by applying an electrical stimulus,
then reducing or removing it, could be prevented by a substance called naloxone
that was known to block the effects of opiates.
Liebeskind established
many other parallels between the kind of analgesia produced by these stimulations
and the effect of opiate medications, thus paving the way to identify descending
pain-control mechanisms, opioid
receptors, and the first endogenous morphines over the following years.