Words have an affective
function as well as an informative one. Memories do not become fixed
biologically unless
there is an emotion associated with them. If someone asks you
to talk about yourself, you will do so largely in terms of the emotions caused
by your relationships with family, friends, and other persons.
Women prefer to talk about how they
feel, while men prefer to discuss impersonal subjects. For women, speaking is
most of all a way of relating to other people, while for men, it is more a way
of transmitting information.
For example, in a study of 6609 people
in five European countries, 66% of the women were the main users of the telephones
in their households, while 76% of the men were the main users of the computers.
This pattern supports the idea that women prefer personal subjects while men prefer
external ones.
Women also make more frequent use of the word “I”
as well as of social words related to persons, while men make more use of “we”
and show more interest in objects and events.
THE CONNECTIONS BETWEEN THOUGHT AND LANGUAGE
Being able to speak means being
able to produce sounds that are recognized by a group as conveying meaning according
to established conventions. Hence a language is a finite system of units of
sound that are combined in a specific order to form words. These words serve as
symbols that are arbitrarily related to objects. And combining these words into
sentences makes it possible to convey an infinite variety of information.
Though language is often regarded as indissociable from thought, it is still
important to distinguish the two. Thought refers to the ability to have ideas
and to infer new ideas from old ones. Language represents a different ability:
the ability to encode ideas into signals for the purpose of communicating.
The most common form of language is oral
communication, in which spoken words are used to express ideas. The basic
components of oral language are called phonemes - elementary units of sound
that are combined in various sequences to form morphemes. A morpheme is
the smallest sequence of phonemes that can carry a meaning that can be isolated
in a sentence in any given language. A morpheme is not the same thing as a syllable:
some morphemes are shorter than one syllable, while others are longer. For example,
in the word "kitchenette" there are two morphemes: "kitchen",
which is two syllables long and the suffix "-ette", which is one syllable
long and conveys the meaning "little".
By combining these phonemes and morphemes,
we can construct as many words as we like (what we call the "dual
articulation" of language). We can then combine these words
with one another to produce a potentially infinite number of sentences.
The lexicon
of a language is the set of all words in that language, its
vocabulary. The syntax is the way that these words are used,
the rules of grammar that enable words to be correctly assembled
into sentences.
But most of all, language is an extremely powerful tool
that remains very closely related to thought, because it enables us to represent—to
“render present”, to evoke—things that exist only in our imaginations,
or that are real but are simply elsewhere in space or time. This is the realm
of semantics: the way that complex combinations of sounds or
words successfully convey meaning.
The
advent of modern
writing could even be said to have introduced yet another level of articulation,
because it requires phonemes to be translated into letters or combinations of
letters. Once communities developed systems of writing, they could transmit their
knowledge more easily from one generation to the next. Cultural
evolution accelerated and facilitated the growth of the arts and sciences.
The information that defined our species no longer was passed on through our genetic
code alone, but also through cultural codes that were handed down from generation
to generation.
Though men may tend not to talk
very much in intimate situations, they can become quite voluble in public. Apparently,
the reason that men tend to speak more and for a longer time in public than women
do is that doing so offers a good opportunity to acquire or confirm their social
status. In contrast, women seem to prefer to express themselves
in the private sphere, which affords greater opportunities to convey emotions.
When a child begins to talk, its
conversation is directed at other people, of course, but also at itself. Piaget
and Vygotsky
called this second type of language “egocentric discourse”, and children
appear to use it to “think out loud”. It is a sort of monologue in
which children seem to explain their actions to themselves, often after having
completed them.
This egocentric discourse, however, seems to gradually
become internalized when the child is 3 to 5 years old. Once this discourse has
become completely internal, children have learned not only how to talk with words,
but also how to think with them.
A number of studies have attempted
to establish a connection between gestures and words (studies involving mirror
neurons, for example). Another study has shown that performative
gestures demonstrating the transition from intention to attention can be observed
in babies 9 to 13 months old. Starting at 14 months of age, articulate language,
for which the gestures laid the groundwork, takes over from them. There thus appears
to be a continuity between gestures and spoken words.
Suppose a mother gives her child
a new pair of shoes, and then somebody telephones the home, speaks to the child,
and asks him what he just got. The child’s reaction will depend on his age.
At age 3, all children will try to show their new shoes to the telephone. At age
4, all or almost all children will use words instead of the object itself.
Children will often go on to elaborate, perhaps saying that the shoes are
a pretty colour, or that it was nice of Mommy to buy them, and so on. In this
way, children begin to use words to act on the mental images and the inner world
of the person with whom they are talking.
LEARNING TO SPEAK
Around the end of their
first
year of life, children realize that they have their own inner psychic landscapes
and that they can share them with other people. At that point children become
part of the world of intersubjectivity, in which they no longer respond solely
to stimuli from the inside, such as hunger, or from the outside, such as their
parents’ smiles, but also to their own conception of other people’s
mental worlds.
Children at this stage have understood that words are
used not just to produce a pleasant flow of sounds, but
are actually symbols used to designate things, often things that are absent.
Thus children are no longer stuck with tangible reality. They can form their own
representation of the world.
This is the psychic context in which children
speak their first words. Their very first words will refer to the people on whom
children imprint (Mommy, Daddy, Grandma, etc.). Next come words about the objects
in their daily lives. Only after that come words about objects that are absent
to the children themselves and absent to other people.
It is around the age of
10 months that a baby usually says its first word, usually “mama”
or“dada”, scarcely distinguishable from the babble around it. A small
word for an adult, but a considerable achievement for the baby, who has thus come
quite a long way since the
moment its parents’ sperm and egg cells met.
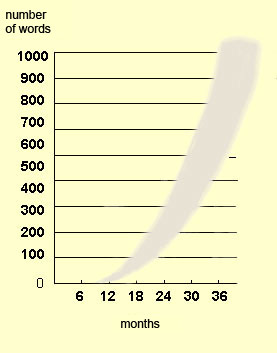
At age
1, the baby knows a handful of words, and at age 18 months, from 30 to
50. Of course, every child develops its vocabulary at its own pace, with the process
generally accelerating so that the child knows over 100 words at 21 months and
over 200 at 2 years.
Approximate number of words in a child’s vocabulary
from birth to age 3. Note the exponential learning curve during these first years
of life.
During this period of
lexical development, children express themselves with individual words in isolation
or with groups of two or three words. These first words are often actually sentences
contracted into a single word, because they do not refer solely to an object,
but to an action or a situation. To interpret these word/sentences properly, you
have to know the context in which they are being used. But gradually, children’s
use of words becomes freed from the present context. Children develop the concept
of object permanence and become able to form a mental image of something without
having it there in front of them.
At age 2,
children have a nearly complete understanding of the language they hear, and when
they want something, they ask for it by formulating a request orally. Children’s
first two- or three-word sentences begin to follow rules of syntax, but do not
include pronouns or articles, and their use of verbs is simplified (French-speaking
children, for example, still use only the infinitive form).
From age
2 to age 5, children master the syntax
of their mother tongue. They do so without ever learning the rules explicitly,
but simply through exposure to the regular structures in other people’s
speech. One proof of this process is that the errors that children make at this
stage are very regular as well. For example, having observed that most English
verbs form the past tense through the addition of the sound “-ed”,
a child might say “I goed” instead of “I went”.
At
about age 3, children’s distortions of words have disappeared
almost completely, and the basic subject-verb-object syntactic structure is in
place. Their vocabulary now includes nearly 1000 words, and they have mastered
the use of the pronoun “I”. Children at this age love listening to
stories and asking questions and are starting to tell about things that they have
seen or done.
At about age 4, children’s words
come in a torrent, composed largely of incessant questions. Children can now talk
about the concept of time (yesterday, today, and tomorrow), and they make more
and more use of prepositions. Thus, at age 4, the primary components of language
are normally in place, and so it is at this age that specific
language disorders can be detected.
At age
5, relative pronouns and conjunctions appear. Children
can conjugate verbs and in general handle language more subtly, even though some
minor imperfections persist. Children also learn to say things in a way that is
more appropriate to the context. They acquire this ability as they gain some distance
from their own perceptions and realize that other people do not necessarily see
the world the same way they do.
At age6,
children use more and more nouns, verbs, and adjectives. Their vocabulary now
totals over 2500 words.
Despite some variations from
child to child, the average age at which these various language abilities are
acquired and the sequence in which they are acquired remain constant from one
culture to the next. Another thing common to all cultures is that the ability
to learn another language diminishes considerably after puberty.
Children acquire the sense of being
themselves at the age of about 5 months, well before they learn to speak. Their
emerging use of language, however, depends on two things: their neurological maturation,
and their cultural and linguistic environment.
For example, when a child
is 3 or 4 years old, the word “dead” means what happens when he points
his finger at an adult and says “Bang! Bang!”: the adult makes a face,
falls on the floor, and stops moving. By the time this child is 5 or 6, though,
his nervous system has matured enough for him to begin to imagine people and things
being very distant physically. “Dead” now means a state of someone’s
being very far away somewhere, for a long, long time. Somewhere between the ages
of 7 and 10, connections form in the child’s brain between the prefrontal
lobe, which is responsible for anticipation, and the limbic system, which manages
memories. Now the child can understand the concept of time, and the word “dead”
refers to something absolute. Thus it takes seven to 10 years for this word to
acquire its “adult” meaning.
This maturation of language
is also affected by genetic and environmental constraints. For instance, a child
who loses her mother at an early age may experience an accelerated maturation
of the word “dead” and understand it completely by age 4 or 5. Conversely,
children who grow up in an environment that is so safe and free of any frightening
ideas as to be almost stifling may remain attached to a very childish conception
of the word “dead” for a longer time. Thus language maturation depends
on both endogenous and exogenous factors.
According to some experts, the Wernicke-Geschwind
model accords too much importance to certain sharply defined areas
of the cortex —Broca’s and Wernicke’s areas— whereas increasingly,
it is being found that the severity of Broca’s and Wernicke’s aphasias
depends on the extent of the cortex affected by the lesion outside of these areas.
Certain subcortical structures not represented in the Wernicke-Geschwind
model, such as the thalamus and the caudate nucleus, can also influence aphasia.
Strokes that damage both cortical and subcortical structures result in more serious
impairments than strokes that damage cortical structures only.
Lastly,
the fact that stroke patients often recover a substantial portion of their language
functions also indicates that other parts of the brain may compensate for those
that have been destroyed.
In people with Broca’s aphasia,
the inability to communicate is often accompanied by other deficits caused by
the damage to the left frontal lobe. Paralysis of the right side
of the body is the most common example. This paralysis may be severe (hemiplegia)
or slight (hemiparesis).
Another deficit sometimes observed
is apraxia, in which the individual cannot perform certain movements
voluntarily but can perform these same movements automatically (for example, they
may be able to lick an ice cream cone without thinking about it but not be able
to stick out their tongue at will).
In some cases,
the left frontal lobe damage may affect vision, causing hemianopsia—the
loss of part of the field of vision.
All of these problems accompanying
Broca’s aphasia mean that in addition to requiring language re-education,
the patient may need physiotherapy and occupational therapy.
Studies of brain lesions can provide
valuable insights into the mechanics of the brain’s cognitive systems. For
example, such studies have shown that music and language are dissociable. Thus
some aphasics can sing a song such as “Blue Moon” but not can’t
speak the word “moon” in isolation or identify the moon by its name
when they see it up in the sky.
LANGUAGE DISORDERS
There are various types
of language disorders, and they fall into two major categories: those related
to development (dysphasia) and those resulting from acquired
brain damage (aphasia).
The types of dysphasia
that are the least serious and the easiest to treat are the articulation
disorders: errors in the movements of the mouth and tongue that are used
to produce phonemes. Most often, these
errors involve consonants (for example, when a child makes the “d”
sound in place of the “t”).
Lisping (pronouncing
“s” as “th”) is another example of an articulation disorder.
Still others include completely omitting a sound (saying “adio” instead
of “radio”) or replacing one phoneme with another (saying “tat”
instead of “cat”). Articulation disorders do not interfere greatly
with children’s ability to make themselves understood, but can expose them
to ridicule and thus make them unhappy.
Speech delays
are another category of dysphasia. They can be caused, for example, by a child’s
not perceiving certain sounds properly in certain words, even though he or she
is not deaf. In such cases it can be very hard for the child to reproduce these
words accurately. For instance, the child may say “shobel” for “shovel”
or “pease” for “please”.
Other forms of dysphasia
involve disorders in the syntactic component of language. Normally,
this component becomes established naturally around
age 3. But children age 4 or 5 who have this disorder still use incorrect
grammar, speak telegraphically, use personal pronouns improperly, or fail to use
the correct forms of verbs.
The language problems associated with dysphasia
are not insurmountable: they often resolve themselves without therapeutic intervention,
but the children concerned will generally be late in speaking and their language
will generally retain, to varying degrees, some signs of the initial disorder.
One particular kind of dysphasia, dyslexia,
produces difficulties in reading.
Aphasia patients who retain a good
understanding of language and are motivated to learn to speak again have a good
prognosis for recovering their use of language. They may continue to show improvement
for nearly three years after the accident that caused their impairment. On the
other hand, if they have shown no improvement three months after the accident,
then the prognosis is fairly poor.
Anosognosia is
a condition in which patients deny their impairment, be it motor-related (for
example, hemiplegia), memory-related (such as amnesia), or language-related (such
as aphasia). For example, patients with Wernicke’s aphasia may be unaware
that their speech is disorganized or that they are having any trouble in understanding
other people when they speak. The fact that such patients “do not know that
they do not know” makes communicating with them more complicated.
The
two most common general forms of aphasia are Broca’s aphasia and Wernicke’s
aphasia. They are named after the two neurologists who, toward the end of the
19th century, described two
different locations in the brain where lesions caused distinct types of language
deficits.
Broca’s aphasia (also known as motor
aphasia or expressive aphasia) occurs as the result of lesions to Broca’s
area in the left frontal lobe. People with Broca’s aphasia search for words
and speak slowly, in a telegraphic manner. For example, if you ask someone with
Broca’s aphasia “Could you explain what you are doing in hospital?”,
he or she might respond, “Yes. Of course. Me go, um, uh, nine o’clock,
speak… two times…read…wri…, um, write…practice…
make prog…-ress.”
People with Broca’s aphasia mainly
use words that have content, while experiencing difficulty with those that have
only a syntactic function (articles, pronouns, and conjunctions) and with the
endings of various verb tenses. These people also have trouble in distinguishing
the subject from the object in sentences couched in the passive voice, such as
“The student is congratulated by the teacher.” The combined result
of all these problems in people with Broca’s aphasia is to significantly
impair their ability to engage in spontaneous oral communication.
People
with Broca’s aphasia sometimes also suffer from apraxia, or from partial
paralysis of the right side of the body (see sidebar). This may have something
to do with the fact that Broca’s area is located close to other areas
with motor functions in the posterior portion of the frontal lobe.
In people with Broca’s aphasia, understanding of language is generally fairly
well preserved. This is not the case for people with the other common form of
aphasia, Wernicke’s.
Lesions that cause Wernicke’s
aphasia (also known as sensory aphasia or receptive aphasia) occur in
the posterior portion of the superior temporal lobe in the dominant cerebral hemisphere,
generally the left. These lesions reduce understanding of spoken and written language,
because this part of the brain plays a critical role in the relationship between
the recognition of a word and its meaning. Responses to simple instructions, such
as “Place object A on top of object B” show that, unlike patients
with Broca’s aphasia, those with Wernicke’s do not understand what
is being asked of them. They can read such an instruction correctly, but cannot
then perform the action indicated by the meaning of the words.
When Wernicke’s
aphasics speak, their language is littered with jargon, made-up terms, and other
incomprehensible words. Their grammar is often intact, but they misuse so many
words that conversation with them is very difficult and somewhat reminiscent of
Chomsky’s
famous sentence, “Colorless green ideas sleep furiously”.
If you ask someone with Wernicke’s aphasia “What brought you
into the hospital?”, he or she might answer, “Well, I sweat, I’m
terribly nervous, you know, from time to time, I can’t move any more, whereas,
on the other hand, you know what I mean, I have to get a move on, look at everything
that’s happening, and all the rest with it.” Another Wernicke’s
patient, when asked to describe a tortoise, replied, “a torpedo, a frammis
that goes in the garden.” Thus Wernicke’s aphasics speak a strange
mixture of clarity and nonsense, yet do so at a very fluent pace.
Wernicke’s
aphasics do not usually have any of the motor neurological impairments, such as
hemiplegia, that may affect Broca’s aphasics.