Because a memory can be deliberately
recalled or consciously evoked, the psychological concept of remembering has come
to be regarded as a special function of the brain. But there is another way to
look at it: all of our behaviours can be regarded as involving an act of remembering.
The voluntary recollection of an abstract concept would then be only a particular
case of this very general process, a phenomenon related to what we call consciousness.
HOW EXERCISING YOUR MEMORY STRENGTHENS IT
The more we think about
a piece of information that we want to remember and its relations to other concepts
that we already know, the less chance there is that we will forget it. This may
be why forgetting is associated more with episodic
memory than with semantic memory. It is probably easier to draw connections
between the meaning of a new word and our network of existing knowledge than to
draw such connections for any particular episode in our lives.
More
generally, the less any given fact is integrated with our overall personality
and activities, the faster we will forget it. We quickly forget anything that
is not supported by a motivation and does not lead to an action.
Various
theories have been developed with regard to forgetting. They deal with the process
of memorization or the processing of information.
Decline Theory
Like
any biological process, memory deteriorates and becomes more fragmented over time.
According
to the decline theory, forgetting occurs when the memory is not exercised or the
information in question is not retrieved often enough.
This is confirmed
by statistics on the words that people forget in a language. Proper nouns, which
are used less often, disappear first. Next come common nouns, then adjectives
(which are used more often, because they can modify many nouns), then verbs, and
then, lastly, exclamations and interjections.
Defective-Recall
Theory
Forgetting is a disturbance in the retrieval of information,
not in its storage.
According to the defective-recall theory, if you are
momentarily unable to access a piece of information in your memory, the reason
is insufficient encoding, or a lack of relationship to your existing semantic
knowledge, or inappropriate retrieval indexes.
But the stored information
still exists somewhere in your memory, because at some other time, you might suddenly
be able to access it.
Motivated-Forgetting
Theory
According to this theory, there are unconscious mechanisms that
make us forget unpleasant or painful facts.
Indeed, psychoanalysts have
shown that forgetting is often associated with events that have disagreeable or
stressful connotations.
Freud postulated a selective process by which people
reject, or suppress in their unconscious, certain memories associated with past
traumas that would be unbearable to remember. Psychoanalysis is based on the idea
that such suppressed memories have not really been forgotten and can be brought
back to patients’ conscious awareness.
Interference
Theory
According to interference theory, a piece of information is
forgotten because some other piece of information prevents it from being retrieved.
In
retroactive interference, new memories tend to erase older ones. Conversely, in
proactive interference, older memories prevent new facts from being committed
to memory effectively.
Thus, together, retroactive and proactive interference
enable us to update our knowledge of the world. New information can overwrite
some of the older information in our memories, through retroaction, but not all
of it, because proaction prevents it.
Some forms of amnesia are highly
specialized and affect only a limited aspect of memory. One very curious example
is the condition known as prosopagnosia. This rare form of amnesia prevents its
victims from recognizing people’s faces. Whether they see these faces live
or in photos, and even if the faces are those of co-workers or family members
(or even, in the most severe cases, their own faces!), they do not know whom they
are looking at. But this can change if a person whom they are looking at speaks.
Often, people with prosopagnosia can recognize someone’s voice and silhouette,
and the rest of their memory functions normally.
This
deficit piqued certain researchers’ curiosity. They investigated, and learned
that certain neurons in the human brain react only when we see faces, and not
when we see other objects. The researchers explained this very high degree of
specialization as follows. 1) The ability to recognize individuals is very important
in social species such as humans, and humans recognize other humans mainly by
their faces. 2) All faces are constructed according to the same pattern. They
differ only in very slight details, which is why specialized neurons have developed
to recognize such details.
TYPES OF AMNESIA
Amnesias can be divided
into two categories: neurological amnesias (originating from organic lesions)
and psychogenic amnesias (arising from psychic traumas). In both categories, a
number of different syndromes have been clearly identified. Here are some examples.
Neurological Amnesias
Alzheimer’s disease strikes later in life and is characterized by
degeneration of certain neurons in the brain. Memory problems are one of the first
warning signs of this illness. This is what makes Alzheimer’s so hard to
diagnose early. As people get older, many of them start to experience minor memory
losses as a normal phenomenon associated with aging. But for people with Alzheimer’s,
over a few years, all of the various forms of memory fall apart. Episodic memory
(memory of events in their own lives) is first to go. Next comes short-term memory,
then memory of the meanings of words, and then procedural (“how-to”)
memory. In the end, all reasoning, attention, and language abilities are disrupted.
Korsakoff’s
syndrome is caused by chronic alcoholism (possibly because it induces
a vitamin B1 deficiency). The brain damage caused by this syndrome leads to progressively
worsening anterograde amnesia. It may also be accompanied by retrograde amnesia,
in which the newer memories disappear first. People with Korsakoff’s are
often totally unaware of it, and answer questions by confabulating, with a sort
of euphoria that also leads to false memories. But the essential characteristic
is still anterograde amnesia, where immediate memory is preserved, but permanent
new memories cannot be established.
Amnesic ictuses are short amnesic
episodes that occur suddenly and last just a few hours. Their causes are poorly
understood. In people who are over 50 years old but in good health otherwise,
the average ictus lasts six to ten hours and is not accompanied by any permanent
brain damage. But during these episodes, people suffer from major anterograde
amnesia, almost instantaneously forgetting everything that has just happened.
In addition, they may experience retrograde amnesia covering several decades of
their lives.
Psychogenic
Amnesias
The most common form of psychogenic amnesia is that associated
with a violent experience, such as being mugged or raped.
This form
of psychogenic amnesia is often accompanied by a fugue state arising after
an encounter that involves an emotional shock. The police often pick up people
in such states who cannot even remember their names and addresses.
These
people lose their biographical memories, but preserve their semantic and procedural
memories. Their episodes of amnesia can last from a few hours to several days,
or sometimes even months. Such cases are rare, however, though they are often
heavily reported in the media.
Multiple personality disorder, in
which two or more personalities give the impression of co-existing in the same
body, also involves a significant memory disturbance. Each of these personalities
seems to have no access to the memories stored by the others.
This form
of amnesia chiefly affects biographical memories, leaving semantic and procedural
memory accessible to all of the person’s identities. This disorder is believed
to develop as a defence mechanism against childhood deprivation or abuse.
After a head injury at age 9, patient
H.M. suffered from epileptic attacks that did not respond to the medications available
at the time. In 1953, at age 27, he underwent an operation to remove the parts
of his brain that were causing the attacks: the two medial temporal lobes of his
cortex (in other words, the hippocampus and surrounding areas on both sides of
his brain).
The attacks ceased, but the operation
resulted in severe anterograde amnesia that prevented him from learning any new
facts from then on. Patient H.M. described his own state as a kind of waking dream.
He retained all of his intelligence and the memories of his distant past. But
he no longer recognized the doctor who had been treating him for years, he would
read the same magazines over and over, and so on.
Anterograde amnesia,
also known as fixation amnesia, is the inability to remember or recognize new
information or new events that occurred after the amnesia’s onset. Retrograde
amnesia, also known as evocation amnesia, is the inability to remember or recognize
information or events that occurred prior to onset.
The
famous patient H.M., for example (see sidebar), was found to have severe anterograde
amnesia together with less severe retrograde amnesia covering the two years preceding
his brain surgery.
This inability to store new long-term
memories literally froze his personal history and knowledge at the point where
they were at the time of his operation. For example, after his operation, H.M.
could no longer recall a list of words a few minutes after hearing it. He also
had difficulty with new words that were entering the language at the time, such
as “jacuzzi” and “granola”.
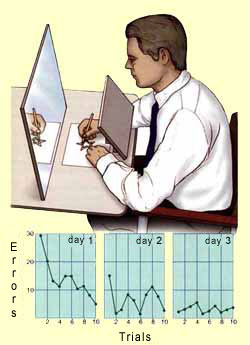
And
yet his short-term memory and implicit memory, as well as his memories of the
distant past, were intact. For example, he could acquire and master new skills,
such as tracking a target or copying an object in a mirror, even though he could
not remember having practiced these skills many times in order to do so. This
separation of his declarative memory from his other forms of memory contributed
greatly to the identification of the major
categories of memory that are recognized today.
The Hanoi
Towers Problem: one of the tests used to assess H.M.’s cognitive abilities
after the operation that caused his amnesia.
Source:
Center for Research, Teaching and Learning - National Technical Institute for
the Deaf
In both of these tests, H.M. improved his
skills over the course of several days, even though each time he took these tests,
he thought that he was doing so for the first time. This shows that despite his
amnesia, he could still acquire certain procedural
memories.