A patient who was followed for thirty
years by the great Soviet neurologist Alexander Luria had the amazing ability
to remember everything. After looking for a few minutes at pages with 30, 50,
or 70 words or numbers, he could repeat them flawlessly one week, six months,
or even 15 years later, without forgetting a thing!
Though he was not insane or autistic, this patient was not entirely normal either.
Among other things, he experienced synesthesia, which means that he had no boundaries
between his various senses. As a result, he experienced some strange associations.For
example, he had the unusual ability to associate a colour, sound, or texture with
a word or number. This gave him a ready means of creating sensory “hooks”
that let him secure words and numbers in his memory permanently.
But this special ability also had some drawbacks. For example, this man had tremendous
difficulty in retaining the meaning of a text that he was learning. To answer
a simple question about the text, he would have to “re-read” the entire
thing in his head! This contrast shows the great power of an ordinary person’s
memory, which encodes the meaning first and foremost. In other words, we may forget
the exact wording of a story, but we remember its essential elements, which is
far more useful in everyday life.
HOW EXERCISING YOUR MEMORY STRENGTHENS IT
Psychologically, forgetting
is the temporary or permanent inability to retrieve a piece of information or
a memory that had previously been recorded in the brain.
Forgetting
differs from amnesia in that forgetting
is usually regarded as a normal phenomenon. Also, forgetting involves specific
pieces of content, whereas amnesia affects a relatively broad category of memories
or wipes out an entire segment of memory.
The
chances of your retrieving a memory depend on many factors, including how well
you have been sleeping and how precisely you labelled this memory in the first
place.
Sleep is a mysterious
phenomenon, but one of its roles appears to be to consolidate the memory traces
stored in the brain over the course of the day.
Thus,
in both animals and humans, an increase in the amount of rapid-eye-movement (REM)
sleep is observed during the night following a learning experience. Conversely,
sleep deprivation adversely affects learning.
Low-frequency
sleep, which occurs mainly at the start of the night, also seems to play a role
in consolidating memories. Some data also suggest that both major phases of sleep
are involved, and that it is the alternation of low-frequency sleep with REM sleep
that produces the beneficial effect.
In
commiting something to memory, just as in any other work, organization
is essential. Two main strategies are available for this purpose: repetition and
elaboration.
In repetition, you take
the piece of information that you are trying to memorize, and you repeat it continuously,
to try to keep it in your short-term
memory, as long as possible.
In elaboration
you associate the new piece of information with other information that you have
already recorded in your long-term
memory. In other words, you incorporate the new fact into a broader, coherent
narrative with which you are already familiar.
This
strategy of elaboration is the basis for many mnemonic devices methods, some of
them very old, for organizing new information so that you do
not forget it.
Le
sommeil, Salvador Dali (1937)
As we grow up, we all experience
various physiological forms of amnesia.
For example,
infantile amnesia is what keeps us from remembering the first three or four years
of our lives. Until children are three or four, they do not form any genuine episodic
memories. But paradoxically, this is the age when they are acquiring a great deal
of knowledge.
Infantile amnesia is not due solely
to the fact that the first years of our lives are the furthest back in time. It
is also due, at least in part, to the lack of language and the immaturity of the
neocortex and other structures in the brain.
TYPES OF AMNESIA
There are several different
types of amnesia, but all can be grouped into two broad categories, according
to the type of trauma that causes them. These two categories are neurological
(or organic) amnesias and psychogenic (or functional) amnesias.
The
damage may result from a cranial trauma (a blow to the head), a cerebro-vascular
accident (a burst artery in the brain), a tumour (if it presses against part of
the brain), hypoxia (lack of oxygen), certain kinds of encephalitis, chronic alcoholism,
and so on.
Psychogenic
amnesias are memory disorders that result from psychological traumas.
Though
these traumas do affect the brain in a certain sense, patients who suffer from
psychogenic amnesia show no detectable brain injury or brain malfunction.
Instead,
the memory loss is caused by some disagreeable event such as chronic stress, intense
fear, rape, incest, etc.
For older people, even if they are
perfectly healthy, it is normal to have a bit more trouble remembering events
from the last few days or weeks. This phenomenon chiefly affects long-term episodic
memory and has little effect on working memory.
Thus,
older people do not lose their semantic
memory (though they may be slower at word-identification tasks) or
their
procedural memory (their memory of how to do things), provided they
have the opportunity to maintain the acquired knowledge through practice.
For
though we now know that our stock of neurons is so large that we can maintain
our memory’s performance to the end of our lives, we also know that memory
needs to be exercised frequently to work properly. People should therefore keep
giving their memory a regular workout as long as possible.
The most famous patient in the history
of memory studies was known by his initials, H.M. He was followed for 40 years
in Montreal by Dr. Brenda Milner. To relieve his attacks of epilepsy, doctors
had removed a part of H.M.’s cerebral cortex, including the hippocampus.
The unexpected secondary effect of this experiment was spectacular: H.M.’s
memories of the episodes of his youth were intact, but he could not acquire the
slightest new long-term memory. People’s faces, his own actions and gestures–everything
disappeared from his mind in just a few minutes, thus confirming the major role
that the missing part of his cortex had played in acquiring new memories. Interestingly,
his procedural
memory (the kind of “know-how” that lets someone get
better at solving the Hanoi Towers puzzle, for example) was not affected at all,
and this supports the hypothesis that various memory systems associated with different
physical structures coexist in the human brain.
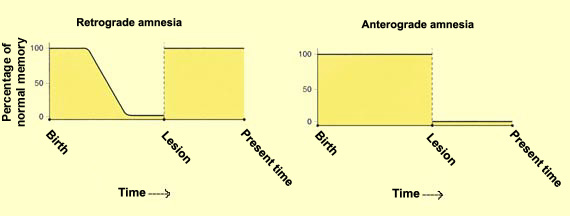
ANTEROGRADE
AND RETROGRADE AMNESIA
Another distinction between
two major types of amnesia is based on whether the patient is forgetting past
facts or forgetting things as they happen.
In retrograde
amnesia, patients forget events that occurred in their lives before they experienced
the trauma, and the oldest facts are the ones least likely to be forgotten.
Recovery
is possible, but the events that occurred closest to the time of the accident
are harder to retrieve and may be lost forever.
Retrograde amnesia is often associated with neurodegenerative
pathologies such as senile dementia and Alzheimer’s disease. In such cases,
the further the disease progresses, the more the memories of the past dissolve.
Anterograde
amnesia is the inability to memorize new facts, and hence the inability to
learn. Following an injury that affects Papez’s
circuit, a person becomes incapable of retaining new facts (explicit
memory). This is sometimes referred to as “forgetting as you go”.
In this type of amnesia, short-term memory and procedural
memory are preserved, because they are independent of Papez’s circuit.
Affected individuals retain their skills but not the memory of having acquired
them (since that would involve episodic explicit memory).
Anterograde amnesia
often occurs following an acute event such as a concussion, a heart attack, oxygen
deprivation, or an epileptic attack.